{kind=link}
Description: PNG image
|
| From: | Richard Terry |
| Subject: | [Gnumed-devel] Past History Comments (was 1.2.3.....) |
| Date: | Wed, 24 Nov 2004 15:10:43 +1100 |
| User-agent: | KMail/1.5.4 |
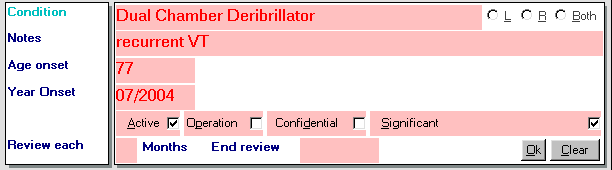
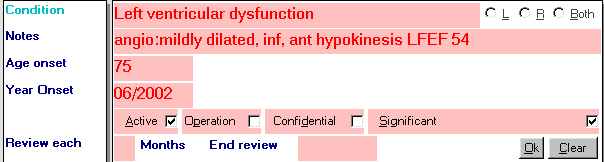
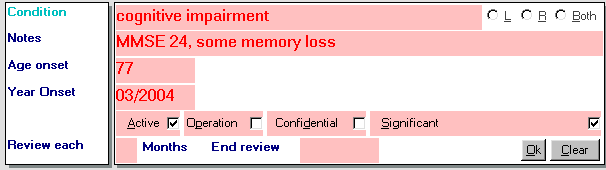
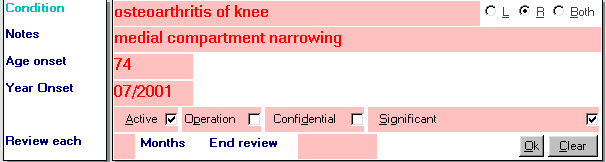
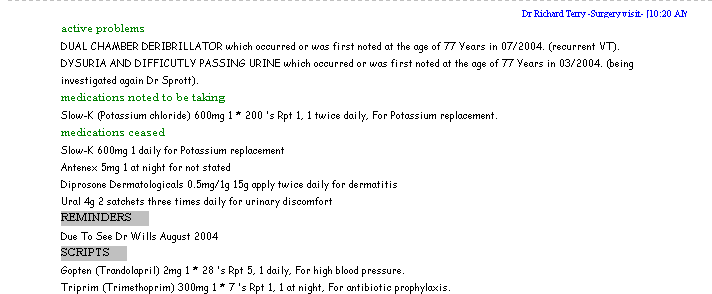
Jim has some good points. My comments below are based on a series of 39622 patient consultations over 7 years, with some 12,000 past history items for various patients entered, and I'd hate to think how many archived/changed. The thing about past history is one needs some sort of detail beyond the diagnosis. A past history being recorded is Not a SOAP note. I've used past history entry since 1997 for all my patients, and I offer the following comments about what does and what does not work with my design. One mportant question with PH is, just what do you want to capture. I.E as Jim has alluded to you need to know just what your needs for data are: - to support your medical record - to be able to re-display when needed yourself - to be able to link to decision support - to be able to link to progress notes - to be able to link to scripts, recalls etc - to be able to pass intelligently on to hospitals/specialists/patient - to be able to give to the patient (incidentally all my patients get a total printout of their medical records each and every time it is updated here) -to be able to support research SQL or otherwise - special cases eg psychiatric history may require quite a bit of detail Here is what I record in my medical records program. Each of these are discrete fields in data_PH table =========================================== PastHistory_ID table key Consult_ID key to consults Age_Onset number could be months or years Age_onset_Units key to lu_units table Description eg Hypertension Notes eg BP's 190/110, 200/150 Side_of_Body key to lu_laterality (0,1,2) ie left,right,both Ozcode disease code Date date condition noted or recorded Active if true this is an active problem Operation yes/no true/false whatever you want Cause_of_death yes/no Confidential yes/no Significant yes/no Deleted yes/no ========================================== You will immediately note that: * a SOAP editor as the list envisages it is not capable of recording this informatiion with this granularity, ie entering the data in ordinary progress notes will not work easily if you want to be able to later modify the way it is displayed, do research etc *a Popup sub-editor will, such as in in SOAP2.py using the skeletal recall example as a substandard and incomplete, but suggestive visual model, or as in the early gnuMed designs I did. when the PH editing area actually existed. *I've attatched some png's from my editing areas in my medical records project to illustrate the sort of data that this captures and will comment on the adequacy/inadequacy/pros/cons of my experience using this below. What works about this granularity: ==================== - If you have a look at the attached png's, you will see that by and large they contain a reasonable amount of information, but not too much, which conveys the essence of the problem, and it is abbreviated enough to be able to pass on to other health care providers. Also it is granular enough to format in several different ways, depending on context. -Laterality is important (if not for the obvious medico-legal reasons!), then for recalling effects of treatments, progress (when often the patient and yourself forget which side of the body the condition was on). -Active or Inactive (and the ability to switch back and forth) speak for themselves. -Operation is useful for reaearch, and is not always obvious from the disease condition -Confidential (I don't want everyone on the bock to know my HIV status or if I have herpes, thank you very much) -Significant -(if not - we really don't need the PH item displayed in PHsummaries - eg the encounter for a Paronychia of the great toe becomes PH but is unlikely to be significant. -Age/Year of onset obviously important if not always accurate What does not work in these examples ======================= 1) The biggest single thing I've found over the 7 years I've been entering data into this is that there is NOT ENOUGH DETAIL in the Notes line and this is a constant source of annoyance to me when entering details of the PH item. I allowed 50 characters for this - arbitrary somewhat - dictated somewhat by the screen design. This is adequate for 90% or consultations, but as with any history it is the few percent where you need more detail that really matter. One can use abbreviations as you can see from my entries, but it is not enough, and besides, anyone of us in general practice who has had to deal with hospital doctors can recall the constant pulling out of ones hair as the resident puts in abbreviations meaningful to them and the hospital system which are meaningless to us. A field of 100 characters would be 99.9% ok, but if using the multi-line SOAP stc control then lengh is not a real issue (except in that one still has to be able to generate a summary for letters etc, and in long term patients the amount of information could become a tome. 2)The rather naive beleif that one could at the time of entering the past history item, allocate a routine period of review, for a particular lengh of time ranging from months to indefinate. Great idea, but singularly the biggest goof in the screen design and functionality because try as hard as I could, and with all the motivation in the world, I could not get it to work in real life practice. Anyway, tis my afternoon off, so I must go now. Regards Richard
![]() ph_je_1.png
ph_je_1.png
Description: PNG image
![]() ph_je_5.png
ph_je_5.png
Description: PNG image
![]() ph_je_3.png
ph_je_3.png
Description: PNG image
![]() ph_je_4.png
ph_je_4.png
Description: PNG image
![]() ph_je_2.png
ph_je_2.png
Description: PNG image
![]() ph_je_6.png
ph_je_6.png
Description: PNG image
| [Prev in Thread] | Current Thread | [Next in Thread] |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}